The Dreaded New Covid Variant
By Tom Woods | Principia Scientific International | December 6, 2021
Here we are nearly two years into this. Some thought: the vaccines will help, because at the very least they’ll calm the fears of the most irrational.
Instead, the vaccines have been used as a weapon to punish, demonize, and even dehumanize dissidents.
And now a new “variant of concern” is here, and plenty of countries that we were solemnly told had “followed the science,” and if only Americans had listened to them we’d be doing, better, etc., are now headed back into lockdown and the adoption of vaccine passports.
(So far, by the way, the numbers for societies with vaccine passports have generally worsened, not improved, but that must be because they haven’t vaccine passported hard enough!)
The South African doctor who first identified the variant reported that there are so far no known deaths from it, and that symptoms have been mild to moderate.
But the hysteria went into overdrive anyway.
Interestingly, though, not everyone from Lockdown Central has bought into that hysteria.
For instance, Brown University’s Ashish Jha, who’s been pretty nasty toward skeptics of government interventions like you and me, had this to say on Twitter:
“Is it possible #OmicronVariant sets us back to square one? No. We have lots of tests that’ll detect Omicron. We have therapies that’ll work. Our vaccines MAY take a hit but will still provide some (may be a lot) protection. We are in a MUCH better place. This isn’t March 2020.”
Even CNN is reporting on academics who caution against panic.
For instance, Robert Garry, a virologist at Tulane University, speaking of Omicron’s mutations, says: “The ones that might affect transmissibility, I mean, I’m just not seeing a whole lot that would give it a real strong advantage over Delta. That’s really the big question. You know, when it gets into a population that has Delta, is it going to out-compete or not out-compete?”
Trevor Bedford is a genome scientist and epidemiologist at the University of Washington and Fred Hutchinson Cancer Center in Seattle. “Given that Omicron lacks so many of the non-spike mutations that have seemed to contribute to Delta’s increased fitness,” he writes, “I wouldn’t be surprised if its intrinsic transmissibility is similar to Gamma.”
One thing we do know:
Applying the same interventions (lockdowns, more masking, etc.) to this new variant that have done nothing to stop previous iterations is a fool’s errand.
And with the protests occurring around the world, and some U.S. employers backing away from mandates, could we be turning a corner?
The prospect of endless boosters also doesn’t bode well for the hysterics. They are losing even some of their original enthusiasts over that, and over mandates for children.
Now is the time to stick the knife in.
Coronavirus Fact-Check #13: “ICUs are filled with the unvaccinated”
OffGuardian | December 6, 2021
It’s become a common meme to refer to ICU’s being “filled” with the unvaccinated, but is there any truth to that?
A few days ago Dr Hillary Jones, whilst being interviewed on Lorraine Kelly, claimed:
90% of people in hospital are unvaccinated”.
Similarly, last week, Kevin Maguire claimed on Jeremy Vine’s show that:
The unvaccinated are filling hospital beds, they’re in ICUs taking up precious resources – there are hospital waiting lists going up because there are so many unvaccinated people in hospitals”
Television presenters and news headlines across the United Kingdom have commonly referred to hospitals being filled with unvaccinated covid19 patients.
As if it could ever be considered evidence of anything, an anonymous “doctor” wrote a piece for The Guardian, which he filled with nameless anecdotal evidence, and emotively headlined:
ICU is full of the unvaccinated – my patience with them is wearing thin
This claim is regularly used as an argument for vaccine mandates, and/or unvaxxed-only lockdowns.
But is it true?
In a word, no.
ICUs are not “full” of unvaccinated covid patients, they’re not even full of covid cases. In fact, they’re not even full at all.
As of last week, NHS England’s own bed statistics reported that England has 4330 available critical care beds, of which 894 (21%) are being used by Covid patients, 2608 (60%) non-Covid patients and 828 (19%) were empty.
So, England’s critical care beds are not even 90% full, let alone 90% full of unvaccinated covid patients.
But let’s be charitable and assume these people misspoke or communicated their point badly. Let’s assume they meant 90% of covid hospitalisations are unvaccinated.
That, at least, is true right? Wrong.
The actual number is 35.4%
According to the UK’s Health Security Agency data (page 31 of this document) 6639 patients were admitted to hospital “with Covid” in the weeks 44-47 of this year. Of those 6639, 2355 were unvaccinated.
So unvaccinated people do not even make up the majority of Covid cases, let alone the majority of ICU admissions in general.
So, even going by the official statistics – which we’ve previously shown are routinely inflated to make the “pandemic” appear frightening – the claim is incorrect.
And that doesn’t even account for the fact that, according to Public Health England, a “Covid hospitalisation” is anyone admitted to hospital for any reason within 28 days of a positive Covid test. This could include people who are admitted to hospital for something else and then happen to test positive while they are there.
We could also discuss the tiny number of hospital beds available in this country, which has more than halved since the 1980s, whilst the population has exploded in that time.
But that’s really an article for another day.
COVID Vaccine Intended To Reduce World’s Population Without Anyone Suspecting Says Leading Doctor

Great Game India | November 27, 2021
The leading doctor credited with improving early treatment of COVID-19 said in a conference that the goal of vaccine transmission campaigns is to “control and kill off a large proportion of our population without anyone suspecting that we were poisoned.”
“The deaths that are meant to follow the vaccinations will never be able to be pinned on the poison. They will be too diverse, there will be too many, and they will be in too broad a timeframe for us to understand that we have been poisoned,” claims Dr. Shankara Chetty.
According to his website, South African family doctor Dr Shankara Chetty, “has treated 7,000 Covid-19 patients without a single hospitalization or death,” combining his insights with his medical background along with his observations of government censorship orders and censorship of medias to support its conclusions.
Joining the Zoom conference as a Doctor, Chetty began by asking the following questions:
“I think the perspective around what is happening is vitally important. We need to understand what the aim is. Everyone knows that there’s inconsistencies, that there’s coercion, but we need to understand why. Why is it there?”
He then identified the “most important” answer to these questions, “pathogen that was causing all the death in COVID illness,” the spike proteins common in both the vaccine and virus designed to be produced in a revivers body.
In my opinion of what’s going on in the world, spike protein is one of the most man-made toxins. And the purpose of this toxin is to kill billions of people without anyone noticing, he went on to add.
“What looks like transpired here, [is] they’ve engineered a virus and put this weapons-grade package onto it called ‘spike protein.’”
The allergic reaction with the initial release of the “most elaborately engineered toxin,” occurs in a small number of people, resulting in more severe cases and death when the vaccine is administered. According to Chetty, this usually happens eight days after the onset of symptoms.
Doctors say that due to the first 14-day international shutdown, people with the COVID-19 virus that caused it are arriving late to the hospital, and these facilities “to engineer death and damage in order to stir all the fear.”
“But the game that they played with this engineered virus was to justify the vaccination of the planet,” he continued.
Chetty added that these injections “expose us to the spike protein for a longer period.”
I often interview doctors online, and Dr. Pierre Kory, Ryan Cole, and Richard Urso have described how long a health risk begins to occur after death from an allergy in the first two weeks.
“We begin to see the endothelial [blood vessel lining] injuries that this vaccine causes with its spike protein, with its influence on its ACE2 receptors. Those are the deaths that are meant to follow. And they will never be pinned onto the spike protein, a very well-engineered toxin,” he said.
“Now spike protein is also a membrane protein. So, the mRNA will distribute this throughout our body. It will be made in various tissues around our body. It will be incorporated into those membranes around our body, and those specific tissues.”
“Those tissues will be recognized as foreign and will trigger a host of autoimmune responses. So, the deaths that are meant to follow the vaccinations will never be able to be pinned on the poison! They will be too diverse, there will be too many, and they will be in too broad a timeframe for us to understand that we have been poisoned,” he went on”
“Now this toxin in the long term is going to get people with pre-existing illness to have those illnesses exasperated,” the doctor explained.
With some toxins, including “bits of HIV protein” within this “definitely engineered” spike protein, Chetty states “people with cancers are going to have their cancers flareup, and they will say they died of the cancer.”
“People with vessel injuries or predisposition like our diabetics and [those with] hypertension are going to have strokes and heart attacks and the rest at varying times, and we’ll attribute those to their preexisting conditions,” he said.
“People are going to develop, over time, autoimmune conditions, the diversity of which will never be addressed by any pharmaceutical intervention because they’re far too targeted.”
“But I think if people understand what the intention is, then they’ll understand why what’s happened has happened. The ill logic, the coercion, the suppression, is all warranted if you understand that there is a bigger plan.
This plan is to make sure that we can control and kill off a large proportion of our population without anyone suspecting that we were poisoned,” the COVID specialist said.
“And so, I think the justification for everything we see is warranted in understanding the endgame,” he concluded.
“I think there’s a huge picture at play; otherwise the vaccines make absolutely no sense. We were sold the vaccine as our savior from the start, and if we look at the science, the science does not play out.”
The last time tony fauci was pushing masks for disease mitigation he was making up his facts and scare mongering too
el gato malo – bad cattitude – december 6, 2021
many of you are probably too young to remember the AIDS panic of the 80’s.
but when it came out, the NIH, with tony fauci leading the charge, was getting literally everything wrong.
they pushed a narrative of fear, vilified the infected, interfered with the development and adoption of effective treatments, and completely misrepresented spread and mitigation.
it’s how we wound up with absolute garbage like this ad:

it’s probably pretty jarring to see, but this is because you now have perspective. at the time, A LOT of people believed this. fear of getting AIDS from public toilet seats was a very real thing. fear of getting AIDS from casual contact or sharing dining or cooking facilities was a very real thing. people worried they might be sitting near a gay person on a bus. the “moral majority” of dingbat tele-evangelists thundered about it daily.
and then, as now, one jumped up bureaucrat with no idea what he was talking about was running around like chicken little screaming of falling skies and grandstanding about non-existent risks to children.
the fact that it was literally the same guy who is still at it should deeply embarrass us all.
i urge you to watch the video and hear him, in his own words. because this is who tony fauci was, and he has not gotten better. he’s just become more powerful and more nastily manipulative and narcissistic.

the appalling inaccuracy and vicious othering of the AIDS campaign is still his bread and butter play. it’s what tony does. only the scale and scope of power has changed.
one day, 20 years from now, people will look back on these rushed and slipshod vaccine approvals and mandates for products that are not at all suited to task and claims about masks and lockdowns and feel sick to their stomachs.
they will not be able to believe how such pseudoscience and rapacious world wrecking doctrine not only got foisted upon the world, but accepted and cheer led by it.
they will, in the light of perspective, marvel that the same man who convinced us that our kids would get AIDS from being near a gay teacher was allowed to generate pretext to close the schools to “protect” children from a disease that poses them almost no risk, a disease they do not contract nor spread serious cases of.
they will be appalled by the suggestion that a non-sterilizing vaccine was forced on them even after the fact that the vaccine does not mitigate spread was known and despite a towering and dangerous adverse events profile that rendered it a clearly of negative benefit to cost proposition to the young and healthy.
in short, they’ll feel just like you probably did looking at that AIDS ad.
think very carefully about just who you are choosing to trust here.
these “experts” do not have track records of being correct or even of being honest.
check the date on this:

they told you not only that these vaccines would stop spread, but that they literally changed the definition of “herd immunity” so that it could ONLY be achieved by vaccines.
then the vaccines failed to stop spread, likely made it worse, and they doubled down on “you need to get vaxxed” in spite of this, pivoting to this bizarre new take of “you need to get vaxxed to save hospital space” which, of course, is ALSO not working. now they want boosters. soon it will be “variant boosters.” if you don’t think annual covid shots are coming, you probably fell for the “did you know the word gullible is not in the dictionary?” trick. twice.
this is not “changing your views when new facts arise” this is “finding new justifications for doing the same thing despite the facts being 180 degrees opposite to what you claimed.”
this is not science, it’s scientology.
it’s the same people making the same mess.
isn’t it about time we broke this cycle?
food for thought.
Nobody can explain why the vaccinated are more likely to get COVID and die
By Steve Kirsch | December 5, 2021
ICYMI, here’s a chart from a recent post by my good friend Mathew Crawford. It basically shows, the more you vaccinate, the more cases and deaths you get.

Critics would argue, “it’s confounded! more elderly are vaccinated.” But the same critics cannot show us this is false. They can only do “hand-waving” arguments that it must be wrong. Not very convincing.
Governments won’t release the data to show vaccinations are safe. I wonder why?
However, we actually agree with the critics that it is confounded but here’s why: governments don’t release the breakdowns publicly so we can’t do any better than this. If the vaccines are so safe, why don’t they release the data to the public to show this?
Is this just a fluke? I don’t think so. Watch this video starting at 7:00. The line goes the wrong way. The more you vaccinate, the worse it gets.
The health authorities are never going to figure this out because it would discredit them. So they have to keep on singing the same tune: “Safe and effective.”
LIFE INSIDE AN AUSTRALIAN COVID PRISON CAMP (CENTRE OF NATIONAL RESILIENCE)
CLOSE CONTACT SUSPECT HAYLEY HODGSON DESCRIBES 14 DAY INCARCERATION
See also:
Camp Australia: The brochure vs reality

Why hide what happens in the first two weeks after vaccination?
Hiding part of the data leads to wrong conclusions
Health Advisory and Recovery Team | December 1, 2021
There have been numerous papers published showing how well the vaccines protect people after the second dose. Some of this effect is an illusion. The effect happens as a result of inaccurate measuring and a phenomenon called survivorship bias.
Survivorship bias happens when a group is compared at two time points, but the members of the group change between the time points. It would be like assessing the quality of a swimming school which favours the technique of throwing people into the middle of the ocean, leaving them for a couple of hours and claiming credit for how well the remaining students can swim. After two hours, the only people left would be the ones who could already swim and possibly a few who learnt to swim the hard way! The poor souls who drowned in the interim don’t even make the count. Attributing the remaining people’s swimming ability to the coach who turned up 2 hours later would obviously give a very misleading picture. Pointing out that no-one drowned in later lessons would be equally misleading in determining the success of the ‘teaching technique’.
With covid vaccination there is a two week period after vaccination that is not included in the data. The rationale given for this is that vaccines take a while to induce antibodies and therefore the first two weeks’ data are not relevant. Obviously this is flawed. What if the vaccines have deleterious effects that are visible straightaway, that have nothing to do with antibody production? An example is the high rate of shingles seen after covid vaccination, suggesting there is a problem with viral reactivation. This may explain why Sars-CoV-2 infection rates are actually higher in the vaccinated than in the unvaccinated in the first two weeks after vaccination.
The effect of eliminating the first two weeks is a misleading data bias. If people become infected and are dying during that period, this needs to be included. The possibility that the vaccine itself may exert an effect on infection rate cannot be overlooked and the entire dataset needs to be included in order to accurately assess effectiveness. By only measuring the period after the higher risk of infection (0-14 days) it is possible to be deceived. Any signal would be missed.
Aside from it being nonsensical in terms of individual risk to remove this period of time, there will also be an impact on the wider community. If the vaccine in fact causes a spike in infections during the first two weeks, this will inevitably increase spread and will lead to an increased number of infections in that community during that time. Therefore, the assessment of the impact of the vaccination programme must include not only the effect on the individual, but the impact on the wider community.
This point is of particular relevance for close-knit communities where many are being vaccinated at the same time, such as schools and in particular communities with a high number of vulnerable people such as care homes and hospitals. What we are effectively doing is ‘speeding up’ the wave of infections (and deaths). Ultimately at the end of the viral season, the same number of people died. Because of excluding the earlier deaths (1-14 days), we are misled into thinking that the vaccines were more effective than they actually were. By only looking at the later period and seeing fewer deaths during that time, the illusion was created that lives were saved. This is evident in data from many countries following vaccine roll-out. The graph below showing the UK versus Europe illustrates this point, as the UK was the fastest to roll out the vaccine. The total number of deaths, represented by the area under the curve, was similar to other countries, but is just compressed into a shorter time period.
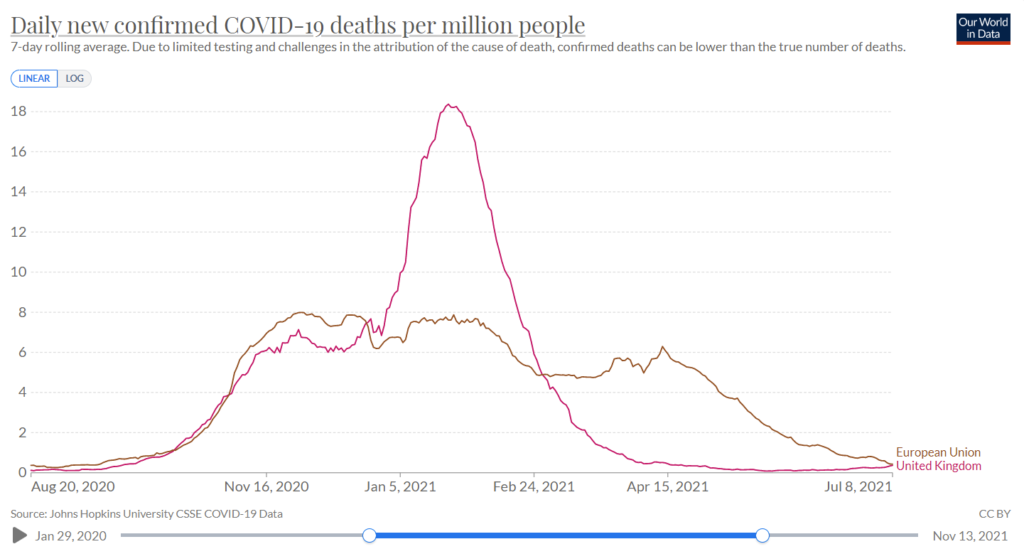
Figure 1: Covid Deaths in winter in UK and the European Union
Let’s now examine some specific examples, e.g. this study of nursing home residents in the United States. The results show that over the course of the study 6.8% of the vaccinated population were infected and 6.8% of the unvaccinated population were infected. However, by deciding that the first 14 days after vaccination should be excluded, the grey area for the vaccinated group is compared to the black and grey area combined for the unvaccinated. Doing so could lead to the claim of 66% vaccine efficacy against infection. The authors of this study were honest enough to share the raw data and did not claim 66% efficacy.
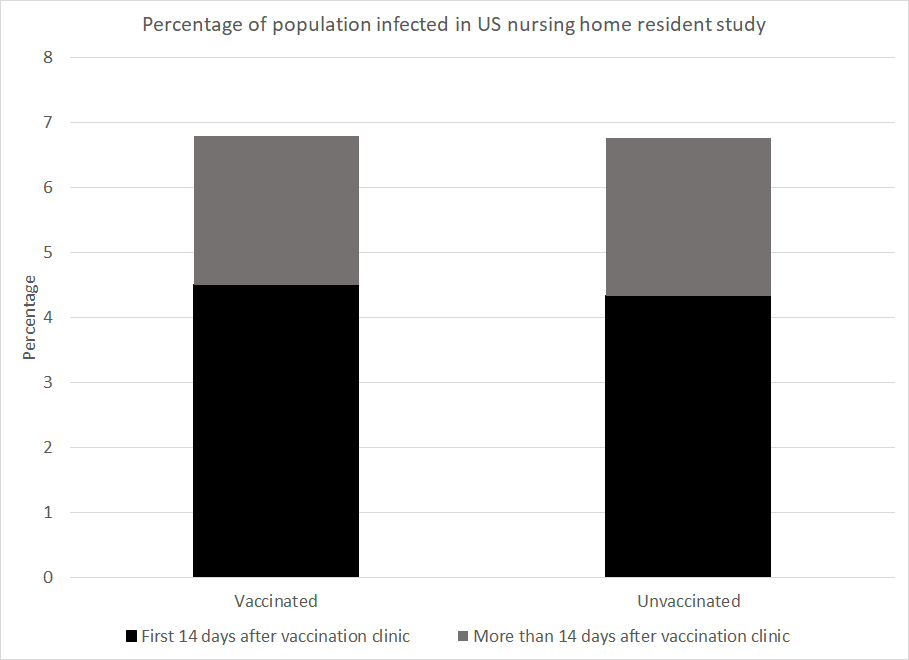
Figure 2: Data from US paper showing the percentage of the nursing home population to be infected by time after the clinic came to their home and by vaccination status
However, numerous studies have relied on this trick to make claims of vaccine efficacy. The most obvious examples of this are the original Pfizer trial study and the AstraZeneca trial.
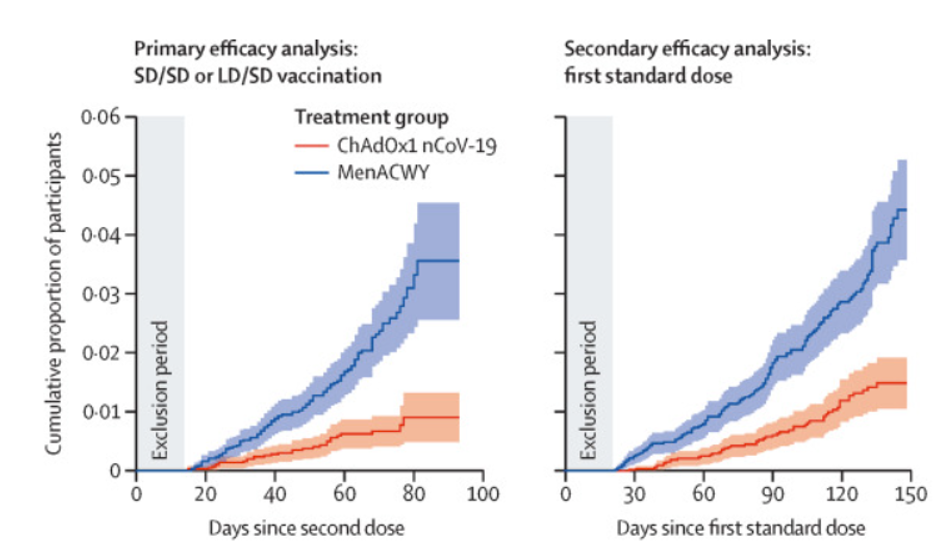
Figure 3: Graph from AstraZeneca trial showing censorship of early period (‘Exclusion Period’)
To take a second example, a Danish paper measured infection numbers in healthcare workers and care home residents. Prior to the beginning of the vaccination programme 4.8% of the healthcare workers had been infected and 3.8% of the care home residents had been. The study ended at the end of the Danish winter wave after 95% of the care home residents had been vaccinated and 28% of the healthcare workers had been. Given the worse position at the start and the lower vaccination rate in healthcare workers you might expect that they were worse off overall. However, the percentage infected by the end of the wave was 7.0% among healthcare workers but 7.7% among care home residents.
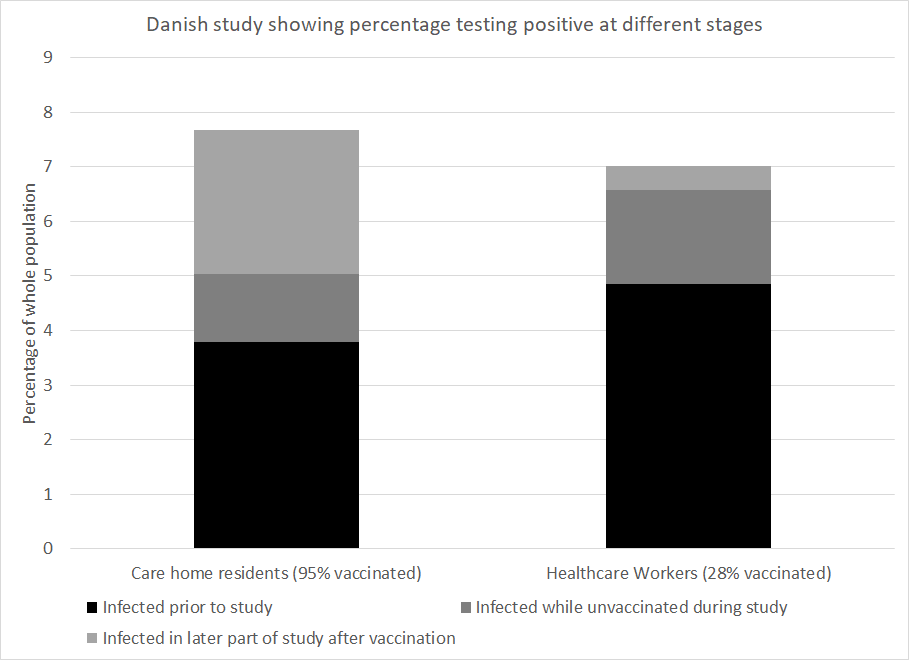
Figure 4: Data from Danish paper showing percentage of population infected among care home residents and healthcare workers
How much of the vaccine efficacy reported in covid research is really a measure of survivorship bias coupled with naturally acquired immunity? This is a critical question. No claim of vaccine efficacy should be made without first addressing this.
UK surgeon remains suspended a year after saying governments are using Covid to control people
By Christina Maas | Reclaim The Net | December 4, 2021
Last year, the UK medical register suspended a consultant surgeon for 12 months pending an investigation by the General Medical Council (GMC) for posting on social media that Covid-19 was being used by elites to control the world.
Colleagues wrote to the organization arguing he should not have been suspended for his personal opinion.
Mohammad Iqbal Adil, a Pakistan-born British doctor, has worked in the NHS for almost three decades. An interim orders tribunal suspended him for a year because of videos he posted on social media.
The doctor expressed “his point of view on the Covid-19 pandemic and the far-reaching effects of the lockdown on the economy, public health and wellbeing,” his campaign page states.
A spokesperson for the GMC at the time said: “The interim orders tribunal imposed an interim suspension on Dr Adil’s registration, following our referral, to protect patients and public confidence. This interim suspension remains in place while we consider concerns about Dr Adil’s fitness to practice.”
Some of his colleagues launched a petition on Change.org calling on the GMC to reinstate Dr. Adil. The petition argues that the GMC should have given him a chance to reflect on the videos “when the entire world is confused about the novel virus.”
The petition also noted that he had a family to support, adding, “UK needs doctors to work. It would not be in the best interest of the public and health system to lose [an] experienced and highly qualified surgeon like him.
“We, the doctors community within [the] UK and across the world, feel that it’s injustice to suspend Mr Adil on his personal point of view on the covid-19 without giving him [a] chance to reflect upon his video before enforcing suspension.
“We request to the GMC to revoke his unfair 12 months suspension . . . and allow him fair chance to work in this country [for the benefit of] the health system, communities, and medical graduates.”
“Dr Adil has been making a stand for freedom of speech for all doctors and nurses to speak their truth without fear of recrimination or persecution,” his campaign page states.
Researchers Acknowledge SARS-CoV-2 Is Gaining Vaccine Resistance
By Dr. Joseph Mercola | December 3, 2021
Looking at the viral evolution of SARS-CoV-2, researchers from the prestigious universities Harvard and MIT have found that the virus not only will continue to mutate and create new variants in the future, but will become resistant to the vaccines as it adapts to humans.
Their study, published December 2, 2021, in the journal Science, shows that the mutations serve as bridges to conferring resistance to neutralizing antibodies. “The severity of the phenotypes we observed in vitro suggest that further evolved variants will more adeptly escape therapeutic antibody neutralization than currently circulating variants of concern, with potential resistance to two-component antibody cocktails,” the study authors wrote.
The scientists urged that “proactively examining the consequences of further viral evolution before the next highly antibody resistant strain emerges is of utmost importance.”
Featured Video

Iran Walks Out On Peace Deal Due To Trump’s Threats
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- Iran to continue IAEA cooperation under existing framework, SNSC decision: Baghaei
- Report highlights US munitions crisis: Missiles cannot be replenished quickly even with al the money in the world
- Iran’s Oil Spigot Could Open Soon But Hurdles Remain
- Trump’s Attempt to End the Iran War Infuriates the Uniparty
- First round of Swiss-hosted Iran-US talks ends with 5 key agreements
- What Is Hay Fever?
- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- Cuban FM blasts Rubio for ‘chronically lying’ about US fuel blockade
- If Americans Knew
- The Republican & Democratic Politicians Trying to Scuttle Iran Agrrement
- Israel’s continued targeting of civilians in Lebanon renders ceasefire meaningless
- U.S. intelligence warns Israel is likely to undermine Iran peace deal, officials say
- In Gaza, Fathers Can’t Promise Their Children Food, Safety, or Even Survival
- This baby joins thousands of Gazans in need of medical evacuation
- Israel Kills Al Jazeera Journalist & Beloved Ecologist: 2 Articles
- Promoters of Israel: Leo Terrell, Ghana, Floyd Mayweather, Van Jones
- Gaza Soccer Player Who Dreamed of Competing in World Cup Can Now Barely Watch It
- Gaza baby loses mom and a leg; Palestinian prisoner tortured to death – Daily Update
- JNS Policy Summit to kick off in Israel
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
